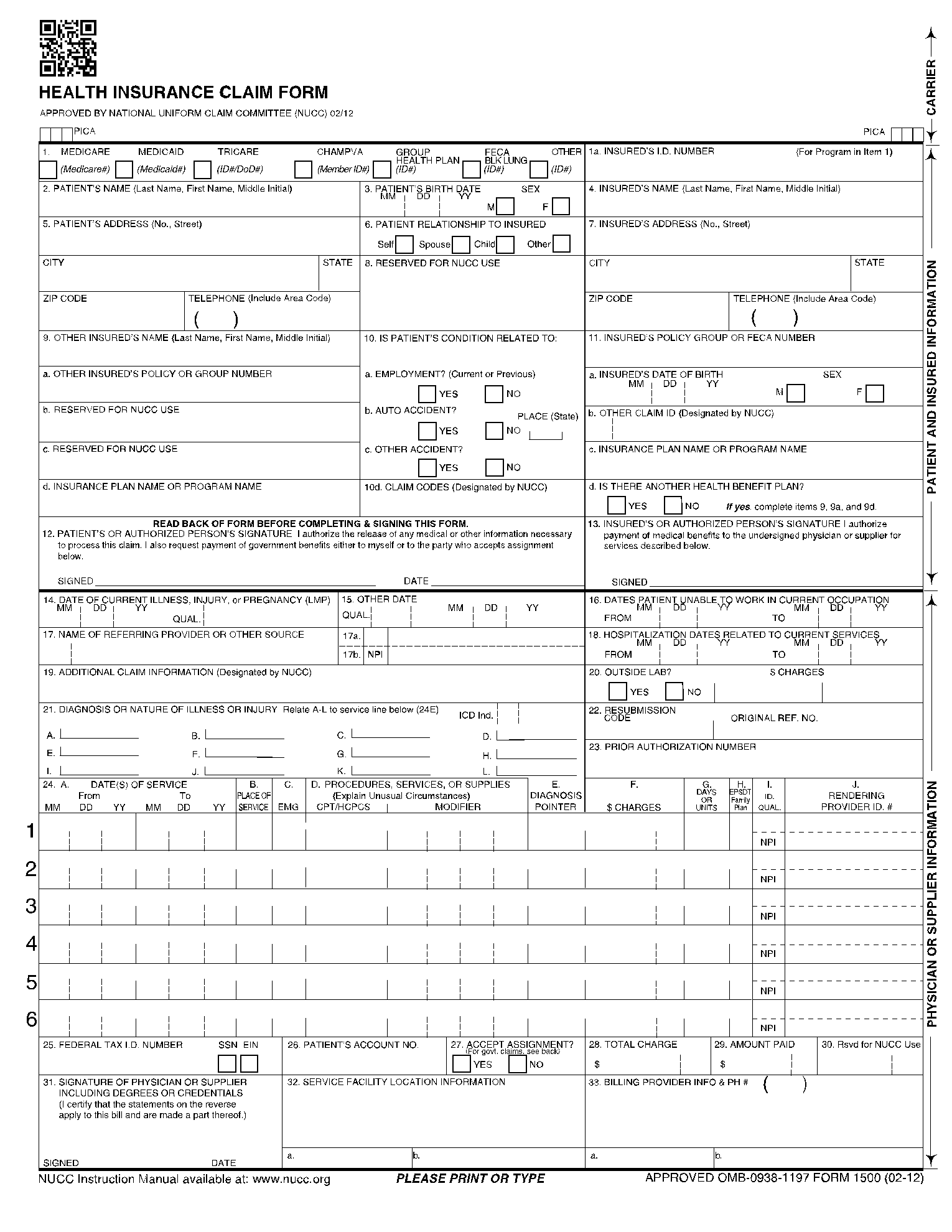
What Is a CMS 1500 Form
This CMS 1500 Form is the universal claim form used by healthcare institutions, physicians, and other providers to submit their claims and invoices to Medicare or Medicaid and private insurance companies. It is filled out by medical care providers and sent to insurance providers.
Information Required on a Health Insurance Claim Form
Before forwarding the health insurance claim form to insurance providers, the following information is key to a successful claim:
- Type of insurance coverage
- Patient's name, address, birth date, and relationship with insured
- Insured's name, address, I.D. number, date of birth, and policy group
- Factors related to the patient's condition
- Insurance plan name
- Date of current illness/injury/pregnancy.
- Name of referring healthcare provider.
- Diagnosis of illness.
- The number of days the patient has been immobilized.
- Hospitalization dates related to the current claim
How to Fill Out a Health insurance Claim Form
The health insurance claim form is an important document providing patients', insured's details and services rendered to insurance companies for processing. We have dissected the paper into a simple step-by-step procedure for filling out the form.
Step 1: Fill Out Insurance and Patient Details
Tick in the appropriate box the type of insurance provider. Next, provide the patient's name, address, and relationship to the insured. You should also indicate factors that may have caused or aggravated the patient's conditions. Other policies held by the insured, the current insurance plan, and claim codes designated by the NUCC should also be stated.

Step 2: Fill Out the Insured's Details
The information required includes I.D. number, name, and address, including telephone number, city, and state. Indicate the insured's policy group, date of birth, claim I.D. as designated by the NUCC. Lastly, in this section, provide the insurance plan or program name and tick appropriately to indicate the existence or lack of any other health benefit plan.

Step 3: Append the Patient's and Insured's Signatures
The patient has to authorize the release of their medical details and other information necessary to process the claim. The insured authorizes payment to the particular healthcare provider for services rendered.

Step 4: Details of the Illness and Hospitalization
Enter the date of initiation of the course of illness, indicate when the patient was unable to work, and name of referring physician, if any. Enter the date when a medical service was furnished concerning the current treatment. Provide the details and the last date when the attending physician saw the patient as additional claim information. Check yes or no to indicate whether an outside lab performed the diagnostic test and indicate their charges. Enter the diagnosis code under the nature of illness and the Quality Improvement Organization or the Investigational Device Exemption number and Post Market Approval number when applicable.

Step 5: Fill Out the Service Lines
Enter the date for each procedure, service, or supply. Under place of service, enter the two-digit code provided in the MCPM and the HCPCS procedure code without a description. Next, enter the diagnosis code reference number as shown in item 21, a charge for each listed service, and enter the number of visits, units of supply, anesthesia minutes, or oxygen volume. Enter the I.D. qualifier 1C in the shaded portion and the rendering provider's NPI number in the lower non-shaded part.

Step 6: Fill Out Billing Details
Enter the provider of service or supplier's Federal Tax ID or Social Security Number, the patient's account number, and check the appropriate box with an (X) to indicate whether or not the provider of service accepts assignment of Medicare benefits. Next is the total amount of charges, the total amount the patient paid, and the signature of the supplier or service provider. Provide the name and address of the NPI service facility that rendered services. Finally, enter the provider's/supplier's telephone number, billing name, address, and ZIP code.

What Is the Health Insurance Claim Form Used For
Healthcare institutions use the form to submit claims to insurance companies to request payment by laying out the list of treatments, medications, fees, tests, and extra costs incurred during treatment. In addition, the form is used to ascertain the patient's demographics, procedures, diagnosis, and supplier or service provider information.
Who Needs a Health Insurance Claim Form
Healthcare service providers, Medicare companies, corporate organizations, and medical insurance companies need the document to claim and process payments for medical treatments undergone by patients. Additionally, companies that provide health care services for their employees need the form.
Additional Health Insurance Claim Form Resources
Below are some additional resources to help you understand this form and fill it:
- Home - Centers for Medicare & Medicaid Services | CMS
- Publications and Forms (opm.gov)
- Government Employee Health Insurance (GEHI) | Government of Bermuda (www.gov.bm)